橫隔膜功能之於核心穩定-下
DIAPHRAGM FUNCTION FOR CORE STABILITY
By Hans Lindgren DC, 9 Jul. 2011
失能的呼吸模式
引起呼吸失能的身心原因往往是不可分開的.因此,呼吸失能也無法被簡單定義.無論是姿勢上、發育上、醫學上或情緒上的原因,呈現出來的失能特徵都非常的相似。失能的呼吸模式包括:上胸廓呼吸並伴隨下肋骨擴張不全或無法擴張。且有不同步或矛盾的呼吸模式 (協調出現障礙)。
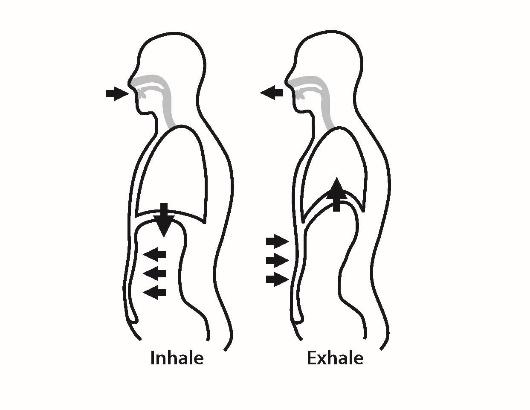
矛盾的呼吸模式包括: 吸氣時,腹部往內收及下段胸廓窄收而非往外擴張。以MRI觀察矛盾呼吸模式在深層呼吸中的橫膈動作:吸氣時,肋骨端的橫膈會往上移動;腳端則會往下移動.吐氣時則呈現相反動作模式。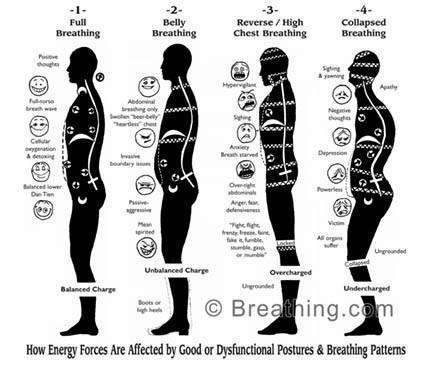
Dysfunctional breathing patterns
Physical and psychological causes of breathing dysfunction can be hard to separate, and dysfunctional breathing can therefore not be simply defined. Whether the cause is postural, developmental, medical or emotional, the presentation is always very similar. Breathing patterns regarded as dysfunctional include upper chest breathing with decreased or absent lateral expansion of the lower ribcage, with a tendency for asynchronous and paradoxical breathing.
During paradoxical breathing the belly is drawn in and the lower ribcage narrows rather than expands during inspiration (13). Paradoxical movement of the diaphragm has been evaluated using MRI during deep breathing which showed an upward movement of the costal part of the diaphragm when the crural part moved downward during inspiration, and the opposite relationship during expiration.
姿勢相關的呼吸失能特徵
胸腔
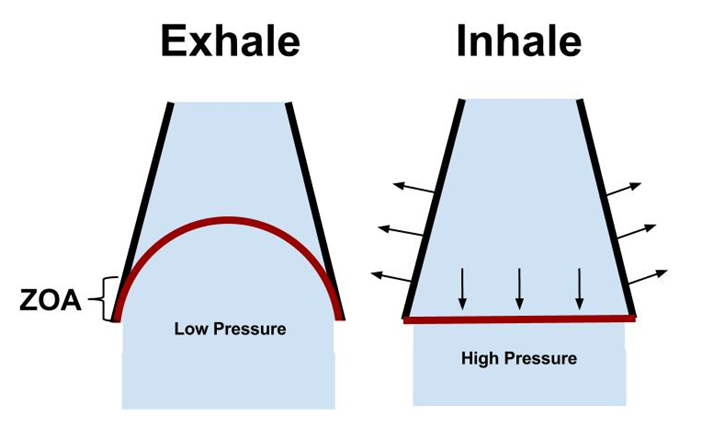
肋骨通常在僵硬、抬高的位置,此位置造成肋骨的外翻。肋骨端的橫膈纖維也被往上拉離原本該有的正常圓頂形狀,進而走向變得更加垂直。在這個位置下,ZOA區域減少,橫膈收縮也被影響。同時,下段肋骨外翻的現象也是常見的問題。
呼吸輔助肌
吸氣時,斜角肌、胸鎖乳突肌、上斜方肌、胸肌等肌肉,因為肋骨過度的垂直活動及肩膀的聳起,常處在高張的狀態。胸腰椎的伸肌群也因為缺乏良好的的核心穩定,也會呈高張狀態來協助維持脊椎穩定。每個呼吸都呈現出肩膀聳起及背部伸直的錯誤動作模式,因此呼吸失能是造成背部、頸部僵硬與疼痛的常見原因。
腹壁肌肉
腹部肌肉不平衡活化伴隨腹內外斜肌、腹橫肌的肌張力減少,在呼吸失能族群中是很常見的。而腹直肌(尤其上段纖維)反呈現高張狀態。呼吸失能的典型特徵為:平躺姿勢下,腹直肌明顯往上抬升而下外側腹壁凹陷空洞。腹部的姿勢肌(tonic muscle)與相位肌(phasic muscle)協同收縮來協助橫膈的呼吸功能。
Postural signs of dysfunctional breathing
The chest
The ribcage is often stiff and held in an elevated position which externally rotates the ribs and pulls the costal diaphragm fibres from its normal dome shaped position to a more straight and vertical position. This position reduces the zone of apposition and thereby the diaphragm’s contraction. Spontaneous flaring of the lower ribs is often observed.
Accessory breathing muscles
Muscles including Scalenes, SCM, upper trapezius and Pectoralis are often hypertonic and over-developed from the increased vertical movement of the ribcage and elevation of the shoulders during inspiration. The thoracolumbar extensor muscles are hyper-tonic attempting to stabilize the spine in the absence of proper core stabilization. Every breath involves a shoulder elevation and a back extension. Breathing dysfunction is a common cause for stiffness and pain in the back and neck.
Abdominal wall
An imbalanced activation of the abdominal wall with reduced muscle tone in the external and internal oblique muscles as well as the transversus abdominis is common. There is usually hyper-tonicity of the rectus abdominis especially in the upper sections. A typical sign of dysfunctional breathing is therefore a marked elevation of the rectus abdominis and concave hollows at the lower lateral abdominal wall in supine. Both phasic and tonic synchronized contractions of the abdominal wall assist the function of the diaphragm during respiration.
無力的腹肌
腹肌無力會弱化橫膈的功能。如果腹肌沒有在橫膈收縮時提供適當的阻力,腹肌會往下移動卻無法明顯增加腹內壓。腹肌對抗橫膈膜收縮的機制,幫助維持ZOA與橫膈圓頂形狀的正常位置。
高張的腹肌
如果腹肌收得太緊,會造成中央肌腱無法下降。在這樣的狀況下,橫膈收縮時會將下肋骨往頭側拉,使肋骨抬起並形成擴張的型態。如果肋骨被收緊的腹肌固定住,則呼吸動作將由上、中胸廓所代償。腹部的凹陷與腹壁僵硬的束縛對理想橫膈活化的發生將造成不良的影響。
Weak abdominals: Abdominal weakness impairs the diaphragm function. If the abdominal wall offers no resistance to the diaphragms contraction it would only displace itself downwards without any distinct increase in IAP. The opposition against the diaphragm contraction performed by the abdominal muscles maintains the important zone of apposition and dome shape of the diaphragm.
Hyper-tonic abdominals: If the abdomen is held too firmly by the abdominal muscles the central tendon cannot descend. Instead, as the diaphragm contracts, it pulls cranially on the lower ribcage which elevates and expands the ribs. If the ribs are completely fixed in place by a strong abdominal muscle contraction the breath will entirely be performed with the upper and middle chest. Abdominal hollowing and a too rigid bracing of the abdominal muscles are therefore counterproductive for ideal diaphragm activation to occur.
理想的腹肌
理想的腹肌運作維持腹腔的形狀與足夠的壓力,同時也提供橫膈足夠的活動,進而讓下肋更充分的擴張。理想的腹內壓是由橫膈、骨盆底肌以及腹壁肌肉協同的運作而維持產生的。吸氣時,離心收縮的腹肌在維持ZOA、橫膈與腹肌之間長度-張力比及軀幹的穩定性與支持都扮演關鍵的腳色。吐氣時,腹肌收縮會增加橫膈長度及圓頂形狀,讓吸氣動作更有效率。
運動時,腹壁肌肉在吐氣的最後階段被強烈徵招,強迫空氣排出肺臟。此強迫吐氣機制會在下次吸氣前增長橫膈膜的纖維,因此可以製造更多的張力來增加吸氣的容積。
Ideal abdominal activity maintains the shape and pressure of the abdominal cavity sufficiently to make the action of the diaphragm more expansive on the lower ribs. The required intra-abdominal pressure is created and maintained by the synchronized activity between the diaphragm, the pelvic floor and the abdominal wall. The eccentric contraction of the abdominal wall during inspiration plays a crucial part in maintaining the zone of apposition and the length to tension ratios between the diaphragm and the abdominal muscles, as well as creating stability and support for the trunk. During expiration, contraction of the abdominal muscles increases the length and dome shape of the diaphragm, allowing for an effective contraction during inspiration
When exercising, the muscles of the abdominal wall are often heavily recruited during late expiration to force air out of the lungs. This forced expiration lengthens the diaphragm fibres prior to the next inspiration contraction and the diaphragm is thereby able to generate more tension which will increase the inspiratory volume.
失能的呼吸模式原因
發育上:出生後第一年不理想的發育會影響穩定系統且造成姿勢上的改變。發育異常影響呼吸的特徵包括:短小僵硬的胸腔(嬰兒胸)、腹斜肌鏈沒有活化足夠造成的下肋外翻、前凸且無力的腹肌常伴隨著腹直肌分離的現象。抬高的胸腔位置以及無力的腹肌大大的減少了橫膈的效能。
醫學上:呼氣末肺容積對橫膈膜收縮及肋骨有很大的影響。慢性阻塞性肺疾病(COPD)、肺氣腫、氣喘等問題常與肺部過度充氣有關(FRC functional residual capacity增加)。過度充氣會造成橫膈縮短、減少圓頂弧度及ZOA區域。研究顯示慢性肺部過度充氣造成橫膈尺寸上的改變,此現象特別發生在ZOA區域。
縮短的橫膈會減少它的力量與效能。橫膈連接下肋骨的纖維是水平走向的(低平橫膈)而非垂直走向。下肋骨走向也變得較水平而不是正常的斜向位置。在這個情況下,橫膈收縮將無法抬起與擴張下肋骨;反在吸氣時,會把下外側肋骨帶往內收。Hodges 研究顯示,呼吸疾病使橫膈與腹橫肌的共同作用功能減少。此外,心臟疾病也影響到呼吸模式。
情緒上:心理上與情緒上的狀態常常改變呼吸的控制。透視影像的研究顯示,在緊張的情況與情緒的壓力下,橫膈膜會呈現高張特徵,像是變得比較扁平與活動降低。
失能的呼吸特徵在一般人占11 % ;占氣喘族群30 %;焦慮族群高達83 %。
呼吸需求增加也會改變呼吸的模式。代償上,將減少呼吸肌肉的功能,轉而維持姿勢。

Causes of dysfunctional breathing patterns
Developmental: non-ideal development during the first year of life affects the stabilization system and often results in postural changes. Signs of developmental abnormalities affecting respiration can be a short stiff chest (baby-chest), flaring of the lower ribs from insufficient activation of the oblique abdominal chains, and a protruding weak abdominal wall often with a diastasis of the abdominal wall present. The high chest position and weakness of the abdominal wall and markedly reduces the diaphragm’s efficiency.
Medical: The end expiratory volume of the lungs has a great influence on the power of the diaphragm contraction and its effect on the ribcage. Conditions like Chronic Obstructive Pulmonary Disease (COPD), emphysema and asthma are often associated with hyperinflation of the lungs where air gets trapped in the lungs. Hyperinflation results in a shortened diaphragm with decreased dome curvature and a reduction of the ZOA (3). Studies have demonstrated that changes in the diaphragm dimensions produced by chronic hyperinflation occur almost exclusively in the zone of apposition.
The shortening of the diaphragm decreases its power and efficiency. The diaphragm fibres attaching to the lower ribcage end up in a transverse orientation (low flat diaphragm) rather than vertical, and the lower ribs shift from their normal oblique position to a more horizontal direction. When the diaphragm contracts during such circumstances it is unable to lift and widen the lower ribcage and instead the lower lateral ribs are being pulled inwards during inspiration (Hoover’s sign (5)). Hodges et al (4) showed that during respiratory disease the co-ordinating function between the diaphragm and the transversus abdominis was reduced. Heart disease also commonly affects the breathing pattern.
Emotional: Psychological and emotional states often alter the respiratory control. Fluoroscopic studies show that in situations of tension and emotional stress the diaphragm shows signs of hyper-tonicity by becoming flattened and immobile.
Dysfunctional breathing is shown to be present in 11% of the normal population, in 30% of asthma sufferers and 83% in people suffering from anxiety (1).
Increased respiratory demand alters the breathing pattern and often reduces the respiratory muscles ability to perform their postural duties (4).
其他正確的橫隔膜呼吸的好處
理想的橫膈呼吸讓橫膈能夠同時執行呼吸及產生足夠腹內壓以提供脊椎支持與穩定的雙功能。此外,橫膈呼吸可增加吸氣容積,促進了肺部通氣量,進而增加血液中含氧量。且下半部肺葉有更多的膨脹,讓更多血液進入下半部肺葉進行氣體交換。
橫膈吸氣會給予腹腔內器官機械效益。失能的呼吸則很淺,主要造成上半部肺葉膨脹。橫膈呼吸同時也提供足夠的腹內壓,藉此維持脊椎穩定。失能的呼吸模式中,呼吸輔助肌(頸部、胸部、背部)不會被徵召。(最後一句話好像怪怪的~)
Additional benefits from proper diaphragm breathing
As mentioned earlier, proper diaphragm breathing allows the diaphragm to perform its respiratory function while simultaneously providing stabilization support for the spine by an increased intra-abdominal pressure (core). Properly synchronized diaphragm breathing also improves the ventilation of the lungs by increasing the inspiratory volume, which increases the level of oxygenation of the blood since the lower lobes expand more, and the majority of the blood sent to the lungs goes to the lower parts.
There is a mechanical effect on the organs in the abdominal cavity when they get pushed downwards during diaphragmatic inspiration - Dysfunctional chest breathing is shallow and mainly expands the top part of the lungs. The posture improves when the lumbar spine properly supported by a sufficient IAP and no accessory muscles (neck, chest and back) are being recruited as in the dysfunctional breathing patterns.
總結
核心穩定的關鍵在於最大化橫膈同時執行呼吸與體態的維持的雙重效益。Kolar研究顯示橫膈在執行姿勢維持會比一般潮氣呼吸時,橫膈會更往下推入腹腔。當橫膈的姿勢維持需求增加時,橫膈在吐氣的位置會比一般呼吸要來得更低。簡單來說,橫膈可自主控制更往下推來增加腹內壓,提供腰椎穩定的支撐。藉由橫膈、骨盆底肌及所有的腹壁肌肉協同作用,來增加腹內壓且同時保持正常的呼吸,這才是核心穩定的真正關鍵。
橫膈在一個比較低的位置時可促進增加腹內壓,腹壁肌肉則提供對抗橫膈的力量。當吸氣時,橫膈收縮,腹部的肌肉會稍微離心收縮來對抗較高的腹內壓,吐氣時,腹肌向心收縮來代償因橫膈離心往上移動而減少的腹內壓力。腹壁肌肉對抗力量的機制可確保橫膈維持理想的長度及圓頂形狀,同時增加橫膈的效能。胸腔的位置及ZOA區域對橫膈的活化也有非常重要的影響。
所以,核心的穩定始於正確的啟動橫膈功能!
Summary
The key to core stabilization is to maximize the diaphragm’s efficiency in performing breathing activity and postural tasks at the same time. Kolar (7) (8) showed that the diaphragm pushes further down into the abdominal cavity during a postural task than during tidal breathing. When the postural tasks become more demanding the diaphragm’s expiratory position is lower than during tidal breathing. In short this means that the diaphragm can be pushed down voluntarily to increase the Intra-Abdominal Pressure (IAP), and provide stabilization support for the lumbar spine. The key to real core stabilization is to maintain the increased IAP while going through normal breathing cycles. This is achieved by the synchronized activity between the diaphragm, pelvic floor and the entire abdominal wall.
The diaphragm then performs its breathing function at a lower position to facilitate a higher IAP. The abdominal wall provides opposition to the diaphragm’s action. When the diaphragm contracts during inspiration the abdominal wall maintains the high IAP through an opposing and slightly eccentric contraction, and during expiration the actions are reversed and the abdominal muscles contract concentrically to compensate for the reduced pressure resulting from the diaphragm’s eccentric upward movement. The opposing activation of the abdominal wall increases the diaphragm’s efficiency of contraction by ensuring the optimal length and dome shape of the diaphragm is maintained. The position of the chest and its effect on the zone of apposition is crucial for proper diaphragm activation.
Core stabilization starts with proper function of the diaphragm!